Andhra Pradesh BIEAP AP Inter 2nd Year Zoology Study Material Lesson 1(b) Breathing and Exchange of Gases Textbook Questions and Answers.
AP Inter 2nd Year Zoology Study Material Lesson 1(b) Breathing and Exchange of Gases
Very Short Answer Questions
Question 1.
Define vital capacity. What is its significance?
Answer:
Vital capacity :
The maximum volume of air a person can breathe in after forced expiration. This includes ERV (Expiratory Reserve Volume), TV (Tidal Volume), and IRV (Inspiratory Reserve Volume) (or) the maximum volume of air a person can breathe out after forced inspiration (VC = TV + IRV + ERV).
Question 2.
What is the volume of air remaining in the lungs after a normal expiration?
Answer:
The volume of air that remains in the lungs after a normal expiration is called ‘Functional Residual Capacity (FRC)’.
FRC = ERV + RV
ERV = 1000 to 1100 ml
RV = 1100 to 1200 ml. So
FRC = 2100 to 2300 ml.
Question 3.
Diffusion of oxygen occurs in the alveolar region only and not in other parts of respiratory system. How do you justify the statement?
Answer:
Alveoli are primary sites of exchange of gas by simple diffusion. Aleveolar region is having enough pressure gradient to facilitate diffusion of gases. Other regions of the respiratory system doesn’t have the required pressure gradient.
High pO2, low pCO2. lesser H+ concentration, low temperature conditions in alveoli favourable for diffusion of O2 ahd formation of oxyhaemoglobin. Solubility of gases as well as thickness of the membrane are also some of the important factors that can effect the ratio of diffusion.
Question 4.
What is the effect of pCO2 on oxygen transport?
Answer:
pCO2 plays an important role in the transport of oxygen. At the alveolus, the low pCO2 and high pO2 favours the formation of oxyhaemoglobin. At the tissues, the high pCO2 and low pO2 favours the dissociation of oxygen from oxyhaemoglobin. Hence, the affinity of haemoglobin for oxygen is enhanced by the decrease of pCO2 in blood. Therefore, oxygen is transported in blood as oxyhaemoglobin and oxygen dissociates from it at the tissues.
![]()
Question 5.
What happens to the respiratory process in man going up a hill?
Answer:
When a man is going up a hill or doing some strenous exercise then there is more consumption of oxygen and resulting in more demand of oxygen. As a result there is an increased breathing rate to fill the gap.
Question 6.
What is tidal volume? Find out the tidal volume in a healthy human, in an hour?
Answer:
Tidal Volume (TV) :
Volume of air inspired (or) expired during normal inspiration (or) expiration. It is approximately 500 ml i.e., a healthy man can inhale (or) exhale approximately 6000 to 8000 ml of air per minute (or) 3,60,000 to 4,80,000 ml per hour.
Question 7.
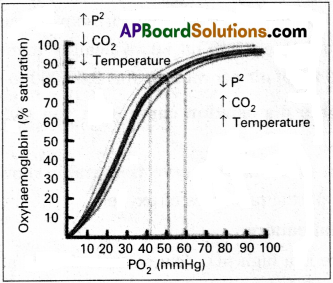
Define oxyhaemoglobin dissociation curve. Can you suggest any reason for its sigmoidal pattern?
Answer:
The oxyhaemoglobin dissociation curve is a graph showing the percentage of oxyhaemoglobin at various partial pressures of oxygen.
Reasons for Sigmoidal pattern :
In alveoli, where there is a high pO2, low pCO2 lesser H+ and low temperature, the factors are all favourable for formation of oxyhaemoglobin. In the tissues where low pO2, high pCO2, high H+ concentration and higher temperature exist, the conditions are favourable for dissociation of oxygen from oxyhaemoglobin under these conditions. Oxygen dissociation curve shift away from the Y-axis and form sigmoid curve.
Question 8.
What are conchae?
Answer:
These are curved bones that make up the upper portion of the nasal cavity. There are different conchae in the nose, such as interior concha, medial concha and superior concha. The nasal concha bones are also referred’to as turbinate pones.
Question 9.
What is meant by chloride shift?
Answer:
Chloride shift:
It refers to the exchange of chloride and bicarbonate ions between erythrocytes and plasma. It is also called Hamburger’s phenomenon.
Question 10.
Mention any two occupational respiratory disorders and their causes in human beings?
Answer:
Occupational respiratory disorders ate caused by exposure of the body to the harmful substances.
E.g.:
1) Asbestosis:
It occurs due to chronic exposure to asbestos dust in the people Working in asbestos factory.
2) Silicosis :
It occurs because of long term exposure to ‘silica dust’ in the people working in mining industries, quarries etc.,
Question 11.
Name the muscles that help in normal breathing movements?
Answer:
Muscles of diaphragm and external inter-costal muscles help in the process of normal breathing movements.
Question 12.
Draw a diagram of oxyhaemoglobin dissociation curve?
Answer:
Short Answer Questions
Question 1.
Explain the process of inspiration and expiration under normal conditions.
Answer:
Inspiration : Intake of atmospheric air into the lungs is called inspiration. It is an active process, as it takes place by the contraction of the muscles of the diaphragm and the external inter-costal muscles which extend in between the ribs. The contraction of diaphragm increases the volume of thoracic chamber in the anterio posterior axis. The contraction of external inter costal muscles lifts up the ribs and sternum causing an increase in the dorso- ventral axis.
The overall increase in the thoracic volume causes a similar increase in the pulmonary volume. An increase in the pulmonary volume decreases the intra-pulmonary pressure to less than that of the atmosphere, which forces the air from the outside to move into the lungs, that is inspiration.
Expiration :
Release of alveolar air to the exterior is called expiration. It is a passive process. Relaxation of the diaphragm and external inter-costal muscles returns the diaphragm and sternum to their normal positions, and reduces the thoracic volume and thereby the pulmonary volume. This leads to an increase in the intra-pulmonary pressure to slightly above that of the atmospheric pressure, causing the expulsion of air from the lungs, that is called expiration.
Question 2.
What are the major transport mechanisms for CO2? Explain.
Answer:
Carbondioxide is transported in three ways.
1. In dissolved state :
7% of CO2 is transported in dissolved state through plasma.
CO2 + H2O → H2CO3.
2. As Carbamino compounds:
About 20-25% of CO2 combine directly with free amino group of haemoglobin and forms Carbamino haemoglobin in a reversible manner.
Hb – NH2 + CO2 → Hb – NHCOO– + H+.
pCO2 and pO2 could affect the binding of CO2 to haemoglobin.
— when pCO2 is high and pO2 is low as in the tissues, binding of more CO2 occurs.
— when pCO2 is low and p02 is high as in the alveoli, dissociation of CO2 carbamino
– haemoglobin takes place, (i.e., CO2 which is bound to haemoglobin from the tissues is delivered at the alveoli)
3. As Bicarbonates :
About 70% of CO2 is transported as bicarbonate. RBCs contain a very high concentration of the enzyme, carbonic anhydrase and a minute quantity of the same is present in plasma too. This enzyme facilitates the following reaction in both the directions.
![]()
At the tissues where partial pressure of CO2 is high due to catabolism, CO2 diffuses into the blood and forms carbonic acid which dissociates into HCO–3 + H+
At the alveolar site where pCO2 is low, the reaction proceeds in the opposite direction leading to the formation of CO2 and water. Thus CO2 is mostly trapped as bicarbonate at the tissues and transported to the alveoli where it is dissociated out as CO2.
Every 100 ml of deoxygenated blood delivers approximately 4 ml of CO2 to the alveolar air.
![]()
Question 3.
How is respiratory movements regulated in man?
Answer:
In human beings the respiratory movements are regulated by neural system.
1. A special centre present in the medulla region of brain, called ‘respiratory rhythm centre’ is primarily responsible for this regulation.
2. Another centre present in the pons of the brain stem called ‘pneumotaxic centre’ can moderate the functions of the respiratory rhythm centre. Neural signal from and this centre can reduce the duration of inspiration and thereby alter the respiration rate.
3. A chemo-sensitive area is situated adjacent to the respiratory rhythm centre which is highly sensitive to CO2 and H+. Increase in these substances can activate this centre, which inturn can send signals to the respiratory rhythm centre to make necessary adjustments in the respiratory process by which these substances can be eliminated.
4. Receptors associated with aortic arch and carotid artery also recognize changes in CO2 and H+ concentration and send necessary signals to the respiratory rhythm centre for necessary actions.
The role of oxygen in the regulation of the respiratory rhythm is quite insignificant.
Question 4.
Distinguish between a) IRV and ERV b) Inspiratory capacity and Expiratory capacity c) Vital capacity and Total lung capacity.
Answer:
a) IRV and ERV:
IRV (Inspiratory Reserve Volume) :
The maximum volume of air that can be inhaled during forced breathing, in addition to the tidal volume. This is about 2500 ml to 3000 ml.
ERV (Expiratory Reserve Volume) :
The maximum volume of air that can be exhaled during forced breathing in addition to the ‘tidal volume’. This is about 1000 ml to 1100 ml.
b) Inspiratory capacity and Expiratory capacity :
Inspiratory capacity (IC) :
The total volume of air, a person can inhale after normal expiration’. This includes tidal volume and inspiratory reserve volume.
IV = TV + IRV
It is about 3000 ml to 3500 ml.
Expiratory capacity (EC) :
The total volume of air, a person can expire after a ‘normal inspiration’. This includes tidal volume and expiratory reserve volume.
EC = TV + ERV
c) Vital capacity and Total lung capacity:
Vital capacity (VC) :
The maximum volume of air a person can breathe in after ‘forced expiration’. This includes ERV TV and IRV (or) the maximum volume of air, a person can > breathe out after forced inspiration.
VC = TV + IRV + ERV
Total lung capacity (TLC) :
The total volume of air accommodated in the lungs at the end of forced inspiration.
This includes RV ERV, TV and IRV
TLC = ERV + IRV + TV + RV (or)
Question 5.
Describe disorders of respiratory system.
Answer:
Disorders of respiratory system.
1) Asthma:
Asthma is a difficulty in breathing caused due to inflammation of bronchi and bronchioles. Symptoms include coughing, difficulty in breathing and wheezing.
2) Emphysema:
It is a chronic disorder in which alveolar walls are damaged and their walls coalesce due to which respiratory surface area of exchange of gases is decreased. One of the major causes of this
3) Bronchitis :
Bronchitis is the inflammation of the bronchi, resulting in the swelling of mucus lining of bronchi, increased mucus production and decrease in the diameter of bronchi. Symptoms include chronic cough with thick sputum.
4) Pneumonia :
The infection of lungs caused by Streptococcus pneumoniae and also by certain Virus, Fungi, Protozoans and Mycoplasmas. Symptoms include inflammation of lungs, accumulation of mucus in alveoli and impaired exchange of gases, leading to death if untreated.
Occupational dissorders :
These are caused by exposure of the body to the harmful substances.
E.g.:
i) Asbestosis:
It occurs due to chronic exposure to asbestos dust in the people working in asbestos industry.
ii) Silicosis :
It occurs because of long term exposure to silica dust.
iii) Siderosis :
It occurs due to deposition of iron particles in tissues.
iv) Black lung disease :
It develops from inhalation of coal dust.
Long Answer Questions
Question 1.
Describe the respiratory system in man.
Answer:
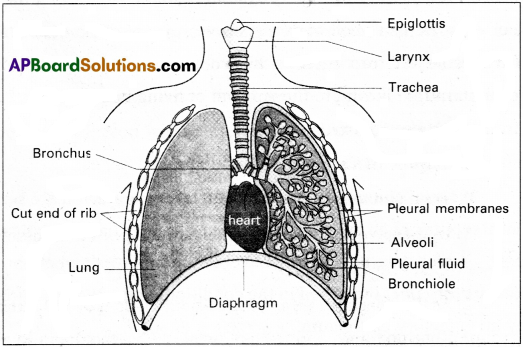
The human respiratory system composed of external nostrils, nasal chambers, nasopharynx, larynx, trachea, bronchi, bronchioles and lungs. It is responsible for the process of respiration that is vital to the survival of living beings.
1) External nostrils :
A pair of external nostrils opens out above the upper lip. They lead into nasal chambers through the nasal passages.
2) Nasal chambers:
They lie above the palate and are separated from each other by a nasal septum. Each nasal chamber can be differentiated into three parts gamely; i) Vestibular part – which has hair and sabaceous gland’s to prevent the entry of dust particles, ii) Respiratory part – involved in the conditioning the temperature, iii) Olfactory part – is fined by an Olfactory epithelium.
3) Naso-pharynx :
Nasal chambers lead into nasopharynx through a pair of internal nostrils. Nasopharynx is a portion of pharynx, the common chamber for the passage of food and air. Nasopharynx leads into oropharynx, and opens through glottis of larynx into the trachea.
4) Larynx :
This is also called voice box or Adam’s apple, connects the pharynx with the trachea. Larynx is the organ of voice as well as an air passage extending from the root of the tongue to the trachea. It is well developed in man. It consist of a) Vocal cord b) Glottis c) Epiglottis.
a) Vocal cord : These are muscular folds that projects from lateral walls.
b) Glottis : Narrow passage between the true and false vocal cords of the larynx.
c) Epiglottis : It is a thin leaf like elastic cartilaginous flap attached to the thyroid cartilage to prevent the entry of food into the larynx through the glottis.
5) Trachea :
Trachea is also called windpipe. It is a straight tube extending upto the mid-thoracic cavity. The wall of the trachea is supported by 16-20 ‘C’ shaped rings of hyaline cartilage. These rings are incomplete dorsally and keep the trachea always open preventing collapse. Internally the trachea is lined by pseudostratified ciliated epithelium.
6) Bronchi and Bronchioles :
On entering the mid thoracic cavity, trachea divides into right and left primary bronchi. Each primary bronchus enters the corresponding lung and divides into secondary bronchi that further divides into tertiary bronchi. Each tertiary bronchus divides and redivides to form primary, secondary, tertiary, terminal and respiratory bronchioles. Each respiratory bronchiole terminates in a cluster of alveolar ducts which ends in alveolar sacs.
7) Lungs :
These are paired, situated in the thoracic chamber which is anatomically an air tight chamber. Lungs are covered by a doubled layered pleura with pleural fluid between them. It reduces friction on the lung surface. The outer pleural membrane is in close contact with the thoracic lining where as the inner pleural membrane is in contact with lung’s surface. The part starting with external nostrils upto the terminal bronchioles constitute the conducting part, whereas the alveoli and their ducts form the respiratory or exchange part of respiratory system. The conducting part transports the atmospheric air to the alveoli, clears it from foreign particles, humidifies and also bring the inhaled air to the body temperature. Exchange part is the site of actual diffusion of and between blood and atmospheric air.
![]()
Question 2.
Write an essay on the transport of oxygen and carbondioxide by blood.
Answer:
Blood is the medium for the transport of oxygen and carbondioxide.
Transport of oxygen :
Oxygen is transported from the lungs to the tissues through the plasma and RBC of the blood. 100 ml of oxygenated blood can deliver 5 ml of O2 to the tissues under norpial condtions.
i) Transport of oxygen through plasma:
About 3% of O2 is carried through the blood plasma in dissolved state.
ii) Transport of oxygen by RBC :
about 97% of oxygen is transported by the . haemoglobin of RBC in the blood. Haemoglobin is a red coloured iron containing pigment present in the RBCs. Each haemoglogin molecule can carry a maximum of four molecules of oxygen. Binding of oxygen with haemoglobin is primarily related to the partial pressure of O2. At lungs, where the partial pressure of O2 is high, oxygen binds to haemoglobin in a reversible manner to form oxyhaemoglobin. This is called oxygenation of haemoglobin.
Hb + 4O2 -» Hb (O2)4.
At the tissues, where the partial pressure of O2 is low oxyhaemoglobin dissociates into haemoglobin and oxygen. The other factors such as partial-pressure of CO2, H+ concentration (pH), and the temperature influence the binding of oxygen with haemoglobin. For example in alveoli high pO2, low pCO2 high H+ concentration lower temperature are favourable for formation of oxyhaemoglobin. In tissues low pO2, high pCO2 high H+ concentration and high temperature conditions are favourable for. dissociation, of oxygen from oxyhaemoglobin.
Transport of Carbondioxide:
Carbondioxide is transported in three ways,
1. In dissolved state :
7% of CO2 is transported in dissolved state through plasma.
CO2 + H2O → H2CO2.
2. As Carbamino compounds:
About 20-25% of CO2 combine directly with free amino group of haemoglobin and forms Carbmino haemoglobin in a reversible, manner.
Hb – NH2 + CO2 → Hb – NHCOO– +H+.
pCO2 and pO2 could affect the binding of CO2 to haemoglobin.
— when pC02 is high and pO2 is low as in the tissues, binding of more CO2 occurs.
— when pCO2 is low and pO2 is high as in the alveoli, dissociation of CO2 carbamino – haemoglobin takes place, (i.e., CO2 which is bound to haemoglobin from the tissues is delivered at the alveoli)
3. As Bicarbonates :
About 70% of CO2 is transported as bicarbonate. RBCs contain a very high concentration of the enzyme carbonic anhydrase and a minute quantity of the same is present in plasma too. This enzyme facilitates the following reaction in both the directions.
![]()
At the tissues where partial pressure of CO2 is high due to catabolism, CO2 diffuses into the blood and forais carbonic acid which dissociates into HCO–3 + H+
At the alveolar site where pCO2 is low, the reaction proceeds in the opposite direction leading to the formation of CO2 and water. Thus CO2 is mostly trapped as bicarbonate at the tissues’and transported to the alveoli where it is dissociated out as CO2.
Every 100 ml of deoxygenated blood delivers approximately 4 ml of CO2 to the alveolar air.